News
-

ISO/IEC 27001 certified!
The Patient Safety Company has received ISO/IEC 27001 certification, showing our commitment to data security! Read more about it here!
Read article -
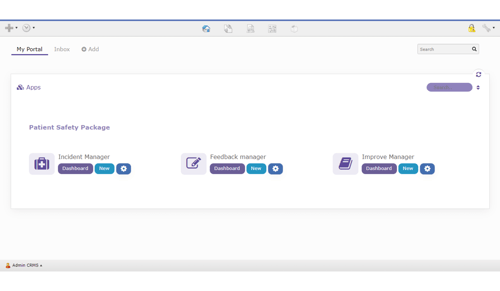
New interface for startpage TPSC Cloud
We proudly present to you our updated TPSC Cloud platform. We changed the search bar, portal layout, inbox and added personal tabs.
Read article -

Safety IQ incident reporting for pharmacies
Under the Safety IQ program, it is mandatory for community pharmacies in Manitoba, Canada to report incidents. TPSC has developed an application for this
Read article -

Sobeys selects The Patient Safety Company for incident reporting
Canada-based Sobeys Pharmacies selected our TPSC Cloud software for incident reporting and quality improvement by all their 400 pharmacies.
Read article -

TPSC joins the Patient Safety event in the Middle East
TPSC joins the Patient Safety event, organized by Informa Markets, for healthcare organizations in the Middle East. Learn more about how we can support you
Read article -

World Patient Safety Day 2021
On 17 September 2021, it's World Patient Safety Day. TPSC supports the call for action to prioritize and address safety in maternal and newborn care.
Read article -
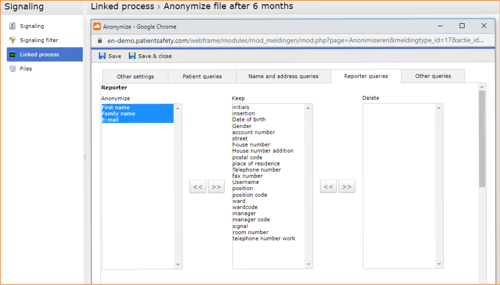
How to anonymize your personal data in TPSC Cloud
The possibility of anonymizing personal data is becoming increasingly important. This article (with video) shows how to do that in our healthcare software
Read article -

TPSC acquired by symplr
symplr acquired The Patient Safety Company. Together we offer a new patient safety and incident management functionality with the symplr GRC platform
Read article -
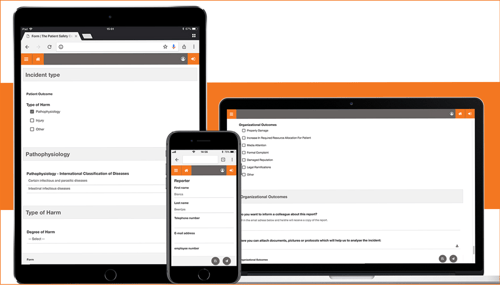
Mobile-first form for data capture
Healthcare staff and patients can report an incident or complaint, submit an idea for improvement, complete a survey, etc., using a tablet or mobile phone!
Read article -
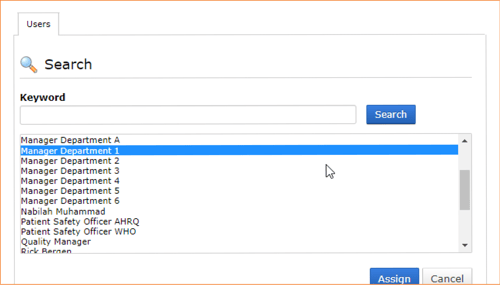
Assign a deputy to follow-up incidents during your vacation
The Patient Safety Company offers a helpful functionality to manage the follow-up responsibility of reported incidents in TPSC Cloud during holiday time
Read article