Data driven healthcare: How to analyse incidents

A systematic analysis and classification of incidents is essential to improve quality and safety in your healthcare organization. There are various methods, which can be divided into two different approaches: retrospective versus prospective.
- A retrospective analysis looks back on what happened. It is a structured approach that leads to finding basic causes of (near) incidents.
- A prospective risk analysis helps you understand how systems or processes can fail. This knowledge can be used to anticipate potential errors.
What is incident analysis in healthcare and why is it important?
Incident analysis involves the systematic review and investigation of adverse events, errors, near misses, and other incidents that occur within healthcare settings. The primary goal is to understand the root causes and contributing factors underlying these incidents. With this understanding it is easier to identify opportunities for improvement and implement preventive measures. Improvement always starts with data analysis.
There are many reasons why incident analysis is important in healthcare. To start with, it improves patient safety. Generally speaking the quality of care will improve when the safety of patients is getting better. By making use of incident data, any healthcare organisation shows that they promote a learning culture. This way of thinking is extremely important in the success of quality improvement. By encouraging open discussion and reflection on incidents, healthcare professionals are able to share lessons learned and identify opportunities for improvement. In the long run this will lead to safer and more effective care.

The solution for risk management
Do you have a good overview of the risks in your organization? Risk managers in healthcare use different ways to report and analyze risks. By using a digital system everyone in your organization can report on risks and this data is accessible everywhere when needed. A risk management system contributes to the quality and safety of your healthcare organization.
In order to learn from incidents and other risks, it is important that all incidents and near incidents are reported. Unfortunately, this is often seen as an additional administrative step that is experienced as difficult and unnecessary.
By using our TPSC Cloud™ solution, every employee and patient can report on risks, through an easy to fill in online form using a desktop or mobile device.
Integrating incident analysis methods using TPSC analysis software
Below we discuss different methods for incident and risk analysis. These analysis methods can be used as inspiration to build your own analysis method, using our software.
- SIRE method
- Ishikawa (fishbone diagram)
- PRISMA analysis (root cause analysis)
- FMEA (prospective risk analysis)
- FRAM-analysis (process visualization)

SIRE Root cause analysis in healthcare
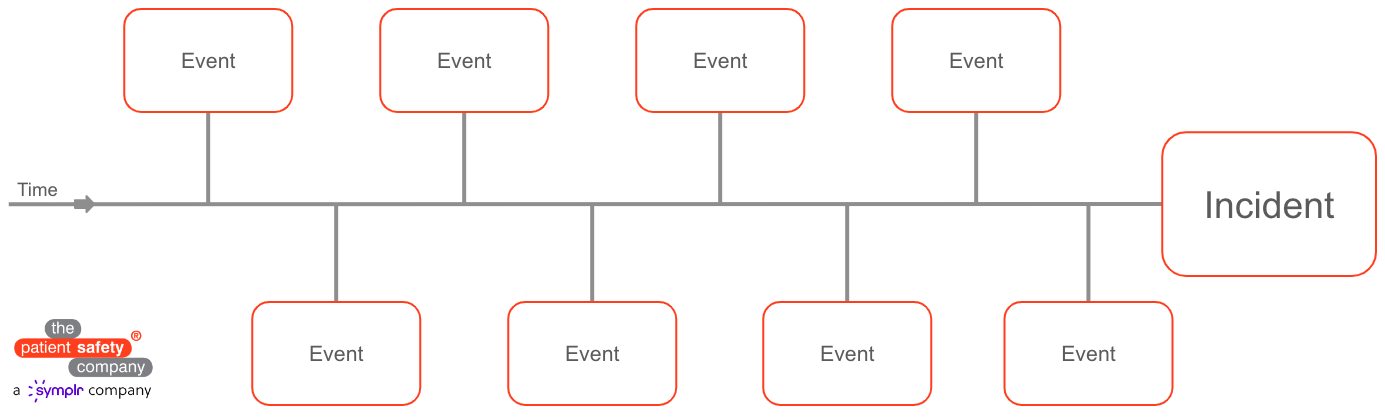
SIRE focuses on incidents with serious consequences or incidents that occur frequently. SIRE offers a toolbox including the following analyses: Timeline analysis, Process analysis and Barrier analysis. The results of SIRE need to justify the relatively high labour intensity.
The SIRE method can be fully implemented within the TPSC CloudTM platform. The specific components can also be chosen as individual analyses.
-
Timeline analysis: provides a chronological record of events and helps with the reconstruction of an (near) incident.
-
Timeline analysis: provides a chronological record of events and helps with the reconstruction of an (near) incident.
-
Process analysis: a three-step tool to describe processes and trace errors.
Ishikawa fishbone analysis in healthcare
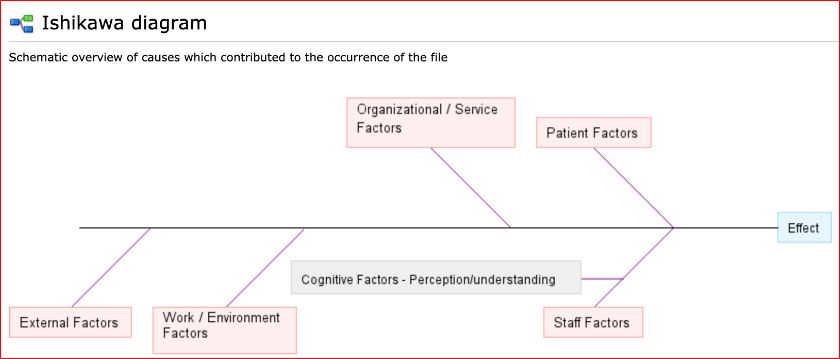
The Ishikawa diagram is a tool for drawing a cause and effect diagram to identify the actual cause of a problem. It is also often referred to as a fishbone diagram. Ishikawa is an accessible method to achieve quality improvement in your organization.
Make an Ishikawa diagram in roughly 3 steps:
-
1Name of the problem and place it at the head
-
2Describe the major causes for the problem on the first branch of the fishbone. These can be different categories such as people, materials, procedures, environment or others determined by yourself;
-
3Divide the major causes in various sub causes by asking yourself why something happens or what causes it.
Incident Management eBook
Read our free eBook for more information about setting up incident management.
-
How do you ensure your organisation learns from incidents?
-
How to modernise to digital incident management?
-
Including tips for analysing incidents.

PRISMA incident analysis in healthcare
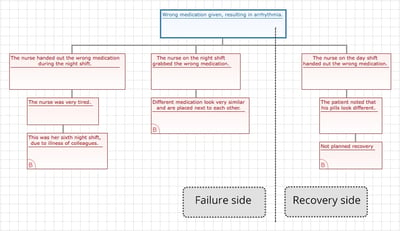
PRISMA stands for Prevention and Recovery Information System for Monitoring and Analysis. This root cause analysis method (RCA) has its origins in the chemical process industry, where the method is used to detect errors and improve processes. Nowadays, PRISMA is also used in other sectors such as healthcare. In a PRISMA analysis, incidents are displayed in a so-called Cause Tree, so that the events can be mapped schematically. In this visual representation the underlying factors and circumstances are easy to read. The in-depth analyses result in effective improvement measures.
With PRISMA, incidents are analysed in 3 steps:
-
1A cause tree is used to describe the incident (see figure);
-
2The root causes, which are identified for each incident by the cause tree, are classified according to technical, organizational and human factors;
-
3A PRISMA profile, consisting of the causes of a large number of incidents, is used to map effective improvement measures with a so-called classification/action matrix.
Incident analysis & improvement using Prisma analysis
It is interesting for a quality officer to keep a database with the root causes that occur regularly. The root causes need to be displayed in terms of percentage, not in numbers. When analysing approximately 30 to 50 incidents with the PRISMA method, it is possible to identify the root causes with a peak and subsequently deploy targeted improvement actions. Following that, new PRISMA analyses will show whether the peak has been reduced and if the improvement actions have worked.
An additional advantage of the PRISMA method is that employees feel they are being listened to after reporting an incident. This method clearly shows that reports are being taken seriously. The question of guilt is less relevant because the deeper underlying causes are made visible. This also has a positive influence on the employees’ willingness to report. In addition, thorough research into the causes and the subsequent communication contribute to awareness.

TPSC software improved with BI functionality
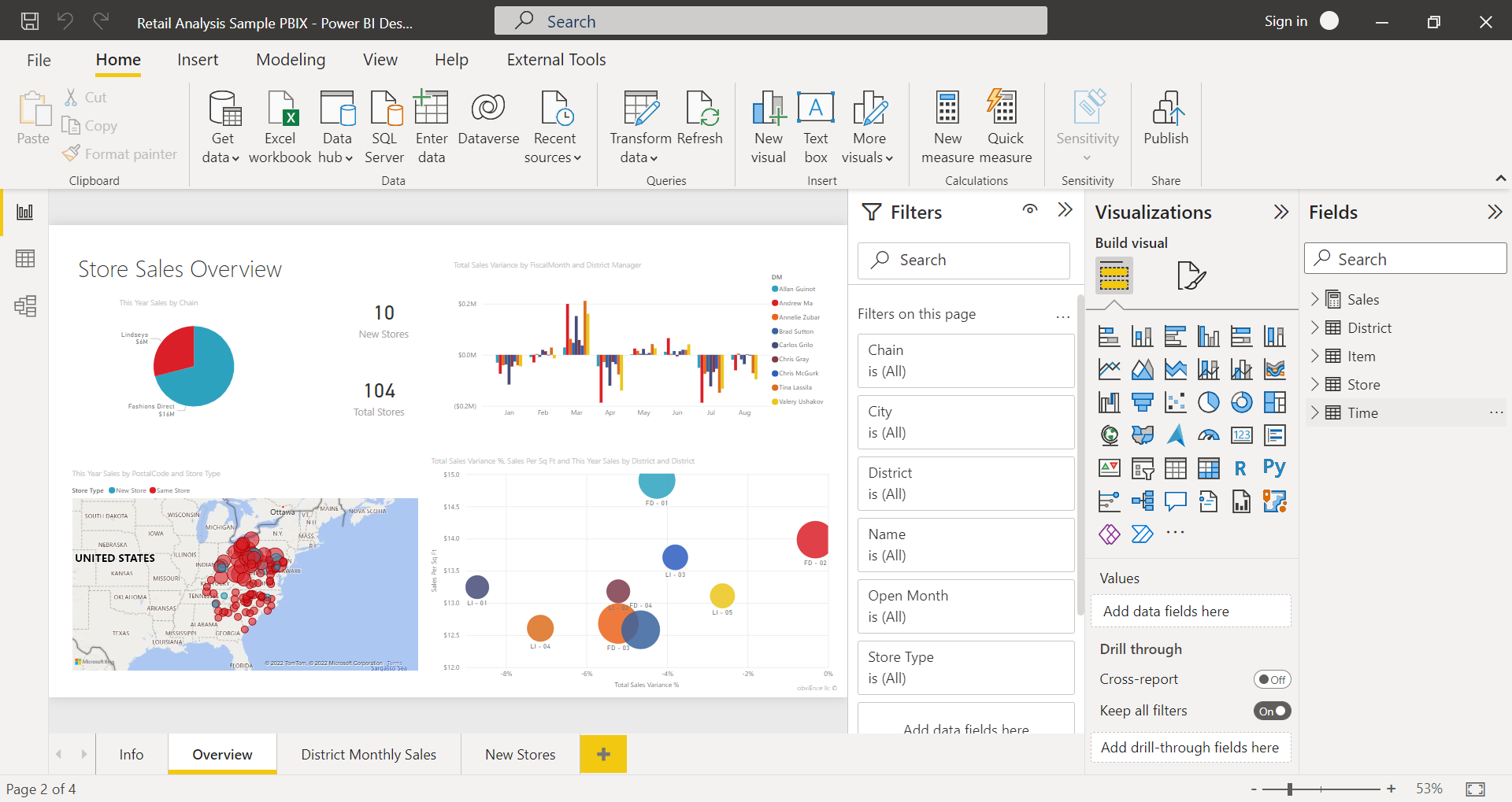
Companies are collecting more and more data about quality and safety. This data is invaluable, provided it is converted into relevant management information. That’s why The Patient Safety Company has integrated Power BI functionalities into our platform.
Users can now use the available data even better, faster and smarter. Compare data, discover cross-connections and trends, zoom in to the smallest detail and create advanced reports! Power BI offers an intuitive, easy-to-use experience; anyone can work with it. Users can make quick data-driven decisions themselves, without being dependent on a business analyst.
Schedule a free online demo or discuss your needs with a specialist.


What is the purpose of a Quality Management System?

Successful implementation of quality management?

How value-based healthcare affects patient safety and satisfaction
