Incident reporting in nursing

In the nursing profession, being at the bedside means you are often the first to witness unexpected events. Accurate incident reporting for nurses is not just a regulatory requirement; it is a fundamental part of providing high-quality care. By documenting near-misses and actual incidents, nurses provide the data necessary to identify systemic issues and prevent future harm to patients and staff alike.

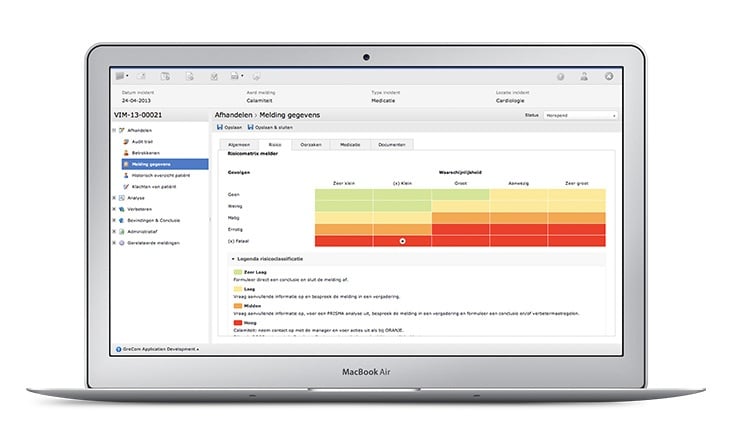
Our incident reporting software for nursing
The TPSC Cloud™ incident reporting software is designed to be as fast and flexible as the teams who use it. We provide a digital incident reporting system in healthcare settings that eliminates the frustration of paper forms and manual data entry.
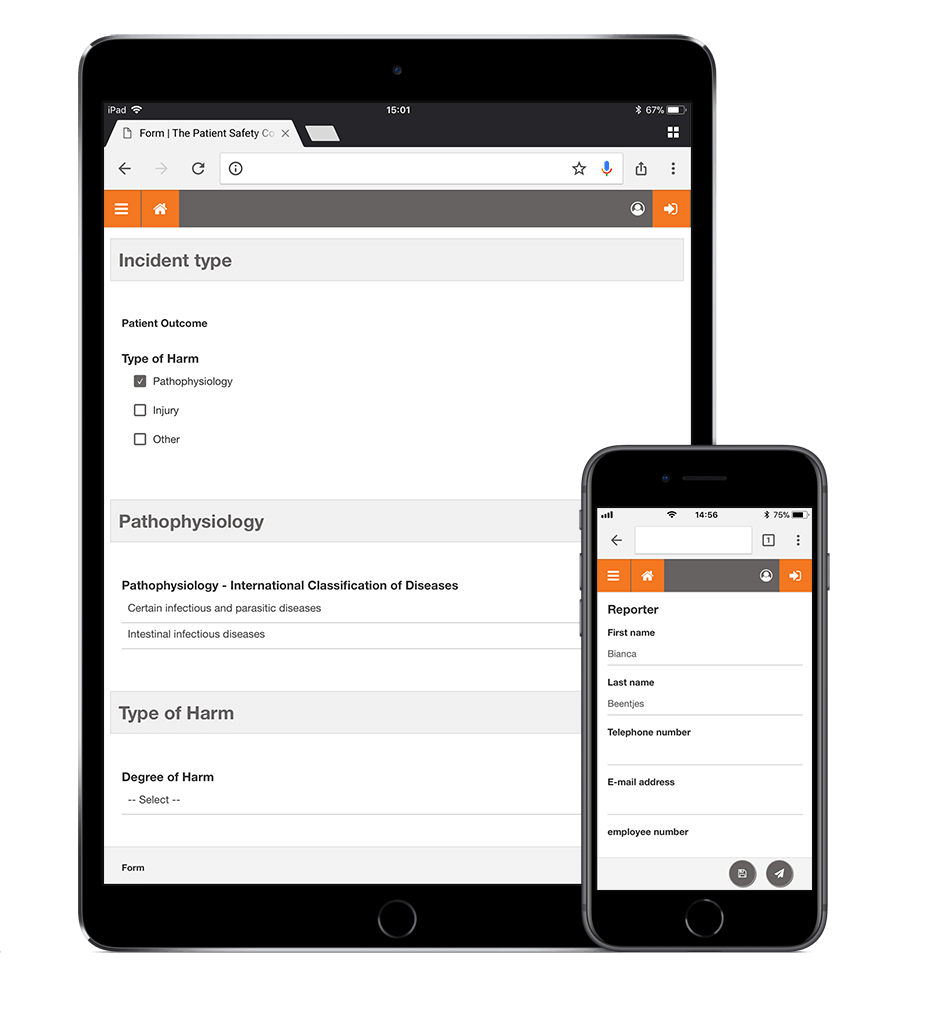
- Easy access: Access our software from any workstation or mobile device in the ward.
- Time-saving forms: Smart, intuitive forms only show relevant questions, allowing you to complete a report in minutes.
- Real-time feedback: Receive automated updates so you can see exactly how your report is being used to improve safety in your department.
Using incident management software to simplify incident reporting
Despite the availability of incident reporting systems, many healthcare organizations still rely on manual, paper-based incident reporting, often using hand-written reports. Manual incident reporting is a time-consuming, costly, error-prone process that has many limitations, including low-quality data and limited flexibility.
Collecting incident data is just the first step in the incident management process. To identify and correct safety problems, the right people have to be able to access, sort, organize and analyze that incident data, something that is very challenging—if not impossible—when using paper reports.
To take full advantage of incident reporting, use incident management software that collects incident data electronically, stores that data in a central database, and analyzes it using proven methods.
Schedule a free online demo or discuss your needs with a specialist.
-
Learn things like creating an incident reporting form
-
See how easily you can analyse incidents and quality-related data

Our valued customers include




